The Center for Judicial Representation under the Ministry of Justice has appealed to the Economic Court of the Eurasian Economic Union (EAEU)
The appeal is based on a request for clarification regarding the application of paragraphs 3 and 4 of Article 98, Section XXVI of the Treaty "On the EAEU," regarding the provision of emergency medical care and other medical assistance. Experts note that the attempt to apply an expansive interpretation of the EAEU legal framework masks the underfunding of the national budget for medical services to the population. Moreover, the stated claims indirectly ignore the participation of humanitarian aid in the healthcare sector coming from Moscow to Bishkek.
The Mandatory Health Insurance Fund (MHIF) of Kyrgyzstan believes that Russian services are acting in violation of Eurasian legislation, according to MHIF Chairman Azamat Mukanov.
— The Russian side is currently violating Articles 96-97 of this agreement by refusing to issue compulsory health insurance to family members of migrant workers. The Kyrgyz Republic has filed a lawsuit against the EAEU, and the case is ongoing. A decision will be made in two weeks,— the official was quoted as saying by 24.kg.

According to the contested clause, social security (except for pensions) for workers of member states and their family members is provided under the same conditions and in the same manner as for citizens of the country of employment. Russian officials, however, rely on Article 10 of Federal Law No. 326-FZ on Compulsory Health Insurance, which only grants the right to a policy to working citizens of the EAEU. Family members of migrants are not included in this category. Compulsory medical insurance is freely available to foreign citizens holding temporary residence permits and permanent residence permits.
In an interview with the Russian publication RBC, Nikita Pyzhikov, head of the Institute of International Economics and Finance at the Russian Foreign Trade Academy, noted significant differences in the development and operation of medical care systems in different EAEU countries.

—Not only do the principles of medical systems differ, but also the scope and level of technological advancement of care provided to insured persons. These issues were not regulated in detail at the drafting stage of the Treaty on the EAEU. The basic regulatory document of the EAEU only clearly stipulates the mandatory provision of free emergency and urgent medical care. The main issues related to compulsory medical insurance are regulated at the national level, — the expert noted.
Moreover, in Kyrgyzstan, even those with compulsory medical insurance are not eligible for free high-tech medical care in cases similar to those covered under Russian protocols. This portion of the cost is covered by the population themselves.
A comparison of the legislation of Kyrgyzstan, Russia, and other EAEU member states reveals a strong commitment by the state to providing health insurance to its population. Belarus, Kyrgyzstan, and Russia hold the strongest positions. However, Kyrgyzstan demonstrates a significant deficit in public funding allocated for the healthcare sector. In turn, thanks to the opportunities offered by Eurasian integration, labor migration to the EAEU significantly reduces the burden on Kyrgyzstan's national budget in the social sector.
An analysis by Business Eurasia of the compulsory medical insurance systems in the EAEU and the mechanisms of Russian-Kyrgyz cooperation in healthcare reveals a trend toward deeper economic integration. A similar challenge previously expanded EAEU legislation on pension provision for migrants.
The healthcare management system in EAEU member states combines centralized state planning and market mechanisms for insurance-based healthcare. The effectiveness of compulsory health insurance directly depends on interdepartmental coordination between government institutions. Each EAEU country has developed its own unique configuration of relevant government bodies.
Russia
In the Russian Federation, the Ministry of Health plays a key role in determining state policy. In turn, the Federal Compulsory Medical Insurance Fund (FCHIF) accumulates insurance premiums and distributes them through territorial funds. The Ministry of Labor and Social Protection coordinates insurance for the working population, and the Ministry of Finance ensures the balancing of budget allocations for non-working citizens.
Kazakhstan
Following the 2017–2020 reform, the Republic of Kazakhstan implemented a compulsory social health insurance (CSHI) system. The Ministry of Health serves as the strategic regulator, and the Social Health Insurance Fund (SHIF) acts as the single purchaser of medical services. The Ministry of Labor and Social Protection of the Population of the Republic of Kazakhstan plays a critical role in verifying citizens' statuses to determine their eligibility for preferential insurance at the state's expense.
Belarus
The Republic of Belarus maintains the most conservative, budget-insurance model, where the role of the Ministry of Health as the direct administrator of budget funds remains dominant. The Ministry of Finance directly finances a network of state institutions. The Ministry of Labor and Social Protection, through the Social Protection Fund (SPF), accumulates funds for pensions and social security, which indirectly support the labor force reproduction system.
Kyrgyzstan and Armenia
The Kyrgyz Republic and the Republic of Armenia are undergoing a profound transformation of their systems. The Ministry of Health of the Kyrgyz Republic and the Compulsory Health Insurance Fund (CHIF) are working closely together to implement the State Guarantees Program (SGPP). The Ministry of Labor, Social Security, and Migration of the Kyrgyz Republic is responsible for integrating migration flows into the social insurance system, which is crucial in the context of EAEU membership.
Institutions in EAEU countries involved in compulsory health insurance processes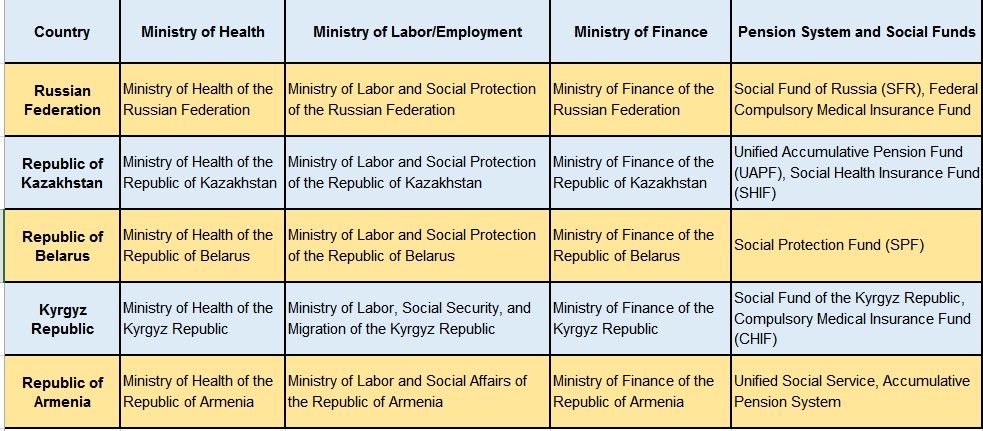
Methodologies for providing healthcare in the EAEU member states vary significantly in terms of funding and the distribution of responsibilities between the state and the citizen. All systems are based on the principle of providing a basic level of healthcare services. However, the mechanisms for implementing this right also vary depending on the country's economic model.
Armenia – Forming a System of Equal Participation
The reform of universal health insurance aims to combine state subsidies for vulnerable groups and mandatory insurance premiums for workers. The current methodology relies on government procurement (budget limits) for medical institutions.
Belarus – State Responsibility
Medical care is financed primarily through general tax revenues. The state is the primary and almost sole payer, ensuring free access to a wide range of services. Citizen participation is limited to tax payments and payment for additional (service or highly specialized) services not included in the social standard.
Kazakhstan – Labor Market Responsibility
The compulsory health insurance system (CHIS) provides for more active citizen participation. Contributions are paid not only by employers but also by employees themselves, as well as individual entrepreneurs and the self-employed. The state retains its role as the payer for 15 privileged categories of citizens. The payment methodology for services is also based on the KNP (comprehensive per capita standard) and payment per case.
Kyrgyzstan – Budgetary Financing Deficit
The Kyrgyz methodology is characterized by a budgetary financing deficit, which has led to the legalization of a co-payment system. The state guarantees program defines the list of services provided free of charge and services requiring partial patient contributions. The state funds a basic package for everyone and an extended package for insured persons (those for whom contributions to the Mandatory Medical Insurance Fund are paid). Particular attention is given to the "Compulsory Medical Insurance Policy," which can be purchased by unorganized groups of the population, including family members of migrants.
Russia
The Compulsory Medical Insurance methodology is based on a per capita financing standard and payment for medical care based on clinical and statistical groups (CSG). The state undertakes to finance assistance to the unemployed population through regional budgets. Individuals participate in the system indirectly through insurance premiums paid by their employers (5.1% of the wage fund). An important feature is the individual's right to choose their health insurance provider and medical facility within the state guarantees program.
Kyrgyz officials' demands regarding the Russian medical services market are largely based on the policy of openness and trust offered by the Russian partnership. Interaction between Russia and Kyrgyzstan in the provision of medical care has evolved from spontaneous migrant requests for emergency care to the systematic inclusion of Kyrgyz citizens in the Russian compulsory medical insurance system. Over the past 15 years, from 2009 to 2024, the number of Kyrgyz citizens treated in Russian medical institutions has steadily increased.
Before Kyrgyzstan's accession to the Eurasian Economic Union (EAEU), access to healthcare for most Kyrgyz in Russia was limited to emergency cases. Statistics from that period recorded between 35,000 and 55,000 visits per year, the majority of which were to ambulance stations and maternity hospitals in large cities. Funding for these services was borne by the budgets of the constituent entities of the Russian Federation as "non-program expenses."
A turning point occurred in 2015, when Kyrgyzstan became a full member of the Eurasian Economic Union (EAEU), and Kyrgyz workers received the same rights to compulsory medical insurance as Russian citizens. This led to the legalization of requests for routine care. Between 2015 and 2019, the number of unique patients from Kyrgyzstan in the Russian healthcare system increased to 80,000-100,000 annually.
In this regard, high-tech medical care (HTMC) is of particular importance. Over 12,000 Kyrgyz citizens have been treated at federal centers for cardiovascular surgery, oncology, and traumatology in Russia over the past 15 years, with a significant portion of these surgeries in recent years financed through insurance mechanisms or intergovernmental cooperation quotas.
During the COVID-19 pandemic, Russian clinics treated Kyrgyz citizens not only through compulsory medical insurance but also as part of anti-epidemic measures. In 2022-2023, the number of migrants and their family members receiving various types of medical care in Russia (from primary healthcare to high-tech) reached a historic high of approximately 160,000 people per year.
Russia is the largest donor of medical technologies and resources to Kyrgyzstan. Over the past 15 years, humanitarian cooperation has evolved from one-time shipments of medicines to large-scale projects to re-equip the republic's entire healthcare system.
Analysis of Russian Federation Humanitarian Aid to Kyrgyzstan (2009-2024)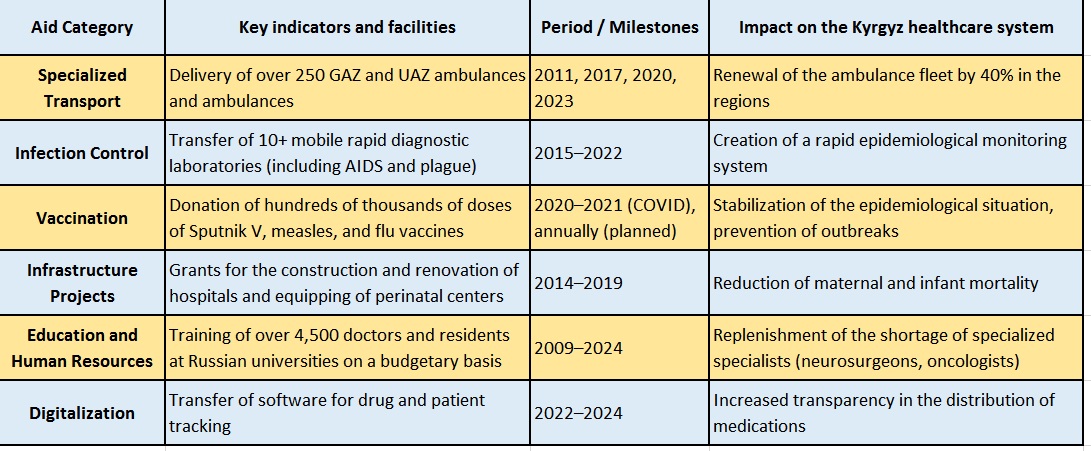
Russia's assistance during the pandemic deserves special mention. In addition to vaccines, Russia sent several teams of volunteer doctors and military medics to Kyrgyzstan, who worked in the "red zones" of Bishkek and Osh, sharing treatment protocols developed at leading Russian research institutes. The Russian-Kyrgyz Development Fund (RKDF) also financed projects to build pharmaceutical plants and diagnostic centers, totaling over $1,20 million.
Legal Regulation of Medical Care in EAEU Legislation
The legal regulation of healthcare in the EAEU is based on a hierarchy of acts that ensure the gradual harmonization of national legislation.
The key document is the Treaty "On the EAEU" of May 29, 2014. Article 98 ("Social Security") stipulates that social insurance (except for pensions) is provided under the same conditions as for citizens of the country of employment. This is the "golden rule" of integration, which removes discriminatory barriers to access to compulsory medical insurance. Article 96 defines the framework for sanitary measures aimed at preventing the spread of infections within the Union.
Decisions of the Supreme Eurasian Economic Council (at the presidential level) set the strategic vector. For example, the Strategic Directions for the Development of Eurasian Economic Integration until 2025 include provisions on the creation of a "digital ecosystem" of healthcare and the implementation of common telemedicine standards.
The Eurasian Economic Commission acts as a supranational regulator. EEC Decision No. 103 approved the "Rules for the Provision of Medical Care to Workers...," which detail the procedure for identifying patients from another EAEU country and the procedure for mutual settlements between funds. The EEC also adopted a set of acts on the formation of a common market for medicines and medical devices, which reduces the cost of drugs by eliminating customs duties and unifying registration dossiers.
The Eurasian Intergovernmental Council focuses on the implementation of specific programs. An important decision was the approval of the Action Plan to Ensure the Sanitary and Epidemiological Welfare of the Population, which provides for a joint response to biological threats and the creation of a unified registry of infectious diseases.
Kyrgyz-Russian Interaction
The activities of the Kyrgyz-Russian Intergovernmental Commission (IPC) are an operational mechanism for structuring bilateral relations. Medical issues have been central to the IPC protocols for the past 15 years.
In 2021-2023, the IPC's decisions were aimed at:
1. Establishing joint medical clusters: Discussing the construction of branches of Russian medical holdings and the National Medical Research Center in Kyrgyzstan.
2. Drug safety: Coordinating the uninterrupted supply of vital medications from Russia in the face of global logistical instability.
3. Mutual recognition of documents: Working on the technical compatibility of Russian electronic medical records and Kyrgyz information systems.
4. Personnel training: A decision was made to increase quotas for Kyrgyz doctors to attend advanced training courses in Russia in the fields of cardiac surgery and rehabilitation.
The IPC places particular emphasis on protecting the health of migrant workers during their stay in Kyrgyzstan (pre-migration training), including conducting medical examinations according to Russian standards in Kyrgyz clinics accredited by Rospotrebnadzor.
Political discourse around healthcare in the EAEU emphasizes not only the social but also the geopolitical significance of cooperation. An analysis of the compulsory medical insurance systems and medical cooperation in the EAEU reveals several key trends and patterns.
First, a shift from "social tourism" to institutional security is underway. While 10 years ago, a Kyrgyz citizen's visit to Russia for treatment was often linked to personal connections or urgent needs, today it is a legitimate process integrated into the compulsory medical insurance system. This reduces corruption risks and the burden on budgets through insurance contributions from employed citizens.
Second, Russia's humanitarian aid to Kyrgyzstan has become a "soft infrastructure." By supplying mobile laboratories and training personnel, Russia is not simply providing assistance but integrating Kyrgyzstan's healthcare system into its technological landscape. This creates a long-term dependence on Russian standards, equipment, and consumables, which, in the context of the EAEU, is a positive factor in stabilizing the region.
Third, the disparity in funding remains a key barrier. Despite legal equality of rights, the actual scope of available care in Bishkek and Moscow differs significantly. This stimulates "medical migration" within the Union, necessitating the development of interstate settlement mechanisms so that insurance premiums paid by Kyrgyz citizens in Russia can be partially returned to the Kyrgyz healthcare system for the treatment of their family members, and vice versa.
Prospects for development lie in digitalization. The creation of a "digital patient profile of the EAEU" will allow doctors in Russia to instantly access the medical records of patients in Osh, which is critical for chronically ill patients and when providing emergency care. The integration of the compulsory medical insurance systems of the EAEU countries will be the final stage in the formation of a single human space on the Eurasian continent.
Text adapted by AI. Should it lack clarity, read the original RU-ver.
Own.info
Business Eurasia